

Introduction: The Hidden Driver of Persistent Pain
Neural sensitization is the process by which the nervous system becomes hyper‑responsive after an injury, causing normal or sub‑threshold stimuli to be perceived as painful. It can be divided into peripheral and central mechanisms. Peripheral sensitization occurs when inflammatory mediators—such as prostaglandins, bradykinin, and cytokines—lower the activation threshold of nociceptors, increasing their firing rate and sending amplified signals to the spinal cord. When this heightened input persists, the dorsal‑horn neurons undergo activity‑dependent changes known as central sensitization: NMDA‑receptor activation, calcium influx, loss of GABAergic inhibition, and neuroimmune signaling all combine to produce wind‑up, allodynia, and secondary hyperalgesia that can outlast tissue healing.
Because sensitization can lock the nervous system into a “high‑volume” state, patients often experience pain that is disproportionate to the original injury, spreads beyond the wound, and interferes with functional recovery. Early identification and targeted intervention are essential. Physical therapy addresses both sides of the equation: manual techniques and graded exercise reduce peripheral nociceptive input, while graded exposure, neuromodulation, and education normalize central processing and restore descending inhibition. By treating neural sensitization, PT helps break the cycle of chronic pain and supports a return to active, pain‑free living.
1. From Injury to Sensitization – What Happens in the Body?
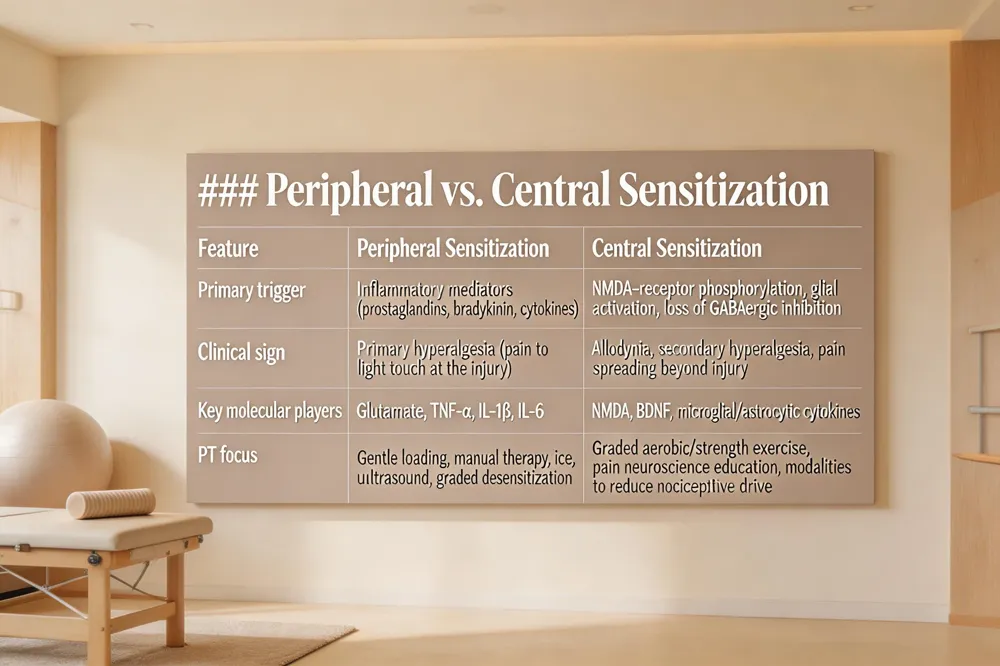 | ||
| Pain starts when nociceptors – the body’s alarm receptors – detect tissue damage and send electrical signals along peripheral nerves to the spinal cord and brain. In the acute phase, inflammatory mediators such as prostaglandins, bradykinin and cytokines lower the activation threshold of these receptors, a process called peripheral sensitization. The result is primary hyperalgesia: even light touch or movement feels painful, and the area may remain sore long after the wound has healed. Physical‑therapy strategies such as gentle loading, manual therapy, ice, therapeutic ultrasound and graded desensitization exercises aim to calm the nociceptors and restore normal thresholds. |
{kind=link}
If the heightened peripheral input persists, the central nervous system adapts. Central sensitization is an activity‑dependent increase in the excitability of dorsal‑horn neurons. NMDA‑receptor phosphorylation, calcium influx, loss of GABAergic inhibition, and sprouting of low‑threshold Aβ fibers expand pain‑processing fields, producing allodynia and secondary hyperalgesia that spread beyond the original injury site.
Key molecular triggers include excess glutamate acting on NMDA receptors, pro‑inflammatory cytokines (TNF‑α, IL‑1β, IL‑6) and chemokines, and the activation of glial cells. Neuro‑inflammation—microglial and astrocytic release of TNF‑α, IL‑1β, BDNF and other mediators—amplifies excitatory signaling and suppresses inhibition, creating a self‑perpetuating pain loop. Therapies that target these pathways (gabapentinoids, NMDA antagonists, graded exercise, education) help reverse maladaptive plasticity and support a return to pain‑free, functional living.
2. Clinical Signs – Recognizing Sensitization in Patients
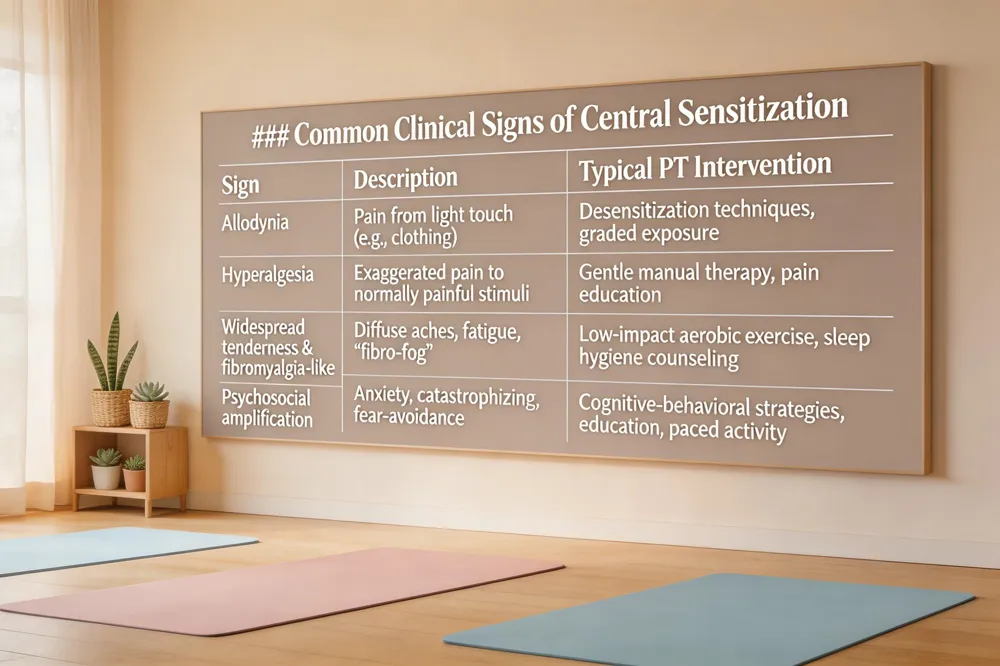 | ||
| Patients with central sensitization often present with a constellation of signs that go beyond the original injury site. Allodynia and hyperalgesia appear as pain from light touch (e.g., a shirt brushing the skin) or an exaggerated pain response to normally painful stimuli, such as a mild pinch. Widespread tenderness and fibromyalgia‑like symptoms include diffuse body aches, headache, gastrointestinal discomfort, and the classic “fibro‑fog" of fatigue, poor sleep, and difficulty concentrating. These symptoms can extend to non‑musculoskeletal systems, reflecting the nervous system’s heightened responsiveness. Psychosocial amplification is common; anxiety, catastrophizing, and stress increase the perception of pain and may trigger a cycle of fear‑avoidance behaviors that further perpetuate sensitization. |
{kind=link}
When pain lingers after tissue has healed, the nervous system remains in a hyper‑alert state—central sensitization—sending pain signals even though the peripheral source is resolved. Scar tissue, residual inflammation, or altered movement patterns can keep nociceptors sensitized, making thorough evaluation and targeted rehabilitation essential. Addressing both the neurophysiological and psychosocial components through education, graded exercise, manual therapy, and coping strategies empowers patients to reset pain pathways and regain functional, pain‑free living.
3. Diagnostic Tools – How Clinicians Identify Sensitization
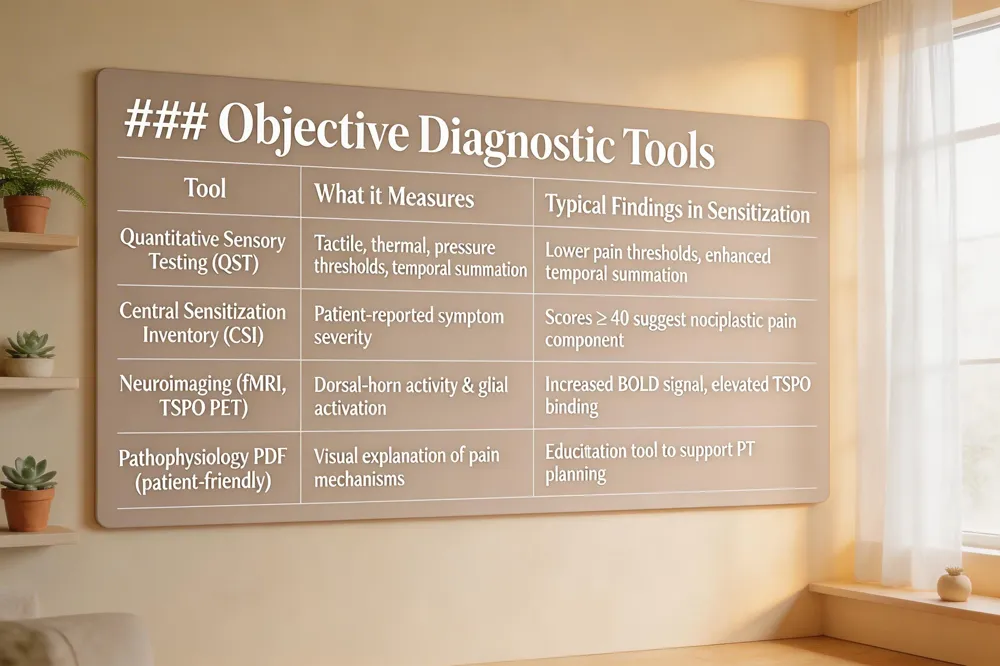 | ||
| Understanding why pain persists after tissue healing begins with identifying neural sensitization. Clinicians use three objective approaches: |
{kind=link}
Quantitative Sensory Testing (QST) – A standardized series of tactile, thermal, and pressure stimuli that maps pain thresholds and temporal summation. Abnormal QST results reveal peripheral and central hyper‑excitability, supporting a diagnosis of sensitization.
Central Sensitization Inventory (CSI) – A patient‑reported questionnaire that quantifies symptoms such as allodynia, fatigue, and brain fog. High CSI scores flag a nociplastic pain component and guide a mechanism‑based treatment plan.
Neuroimaging Biomarkers – Functional MRI, BOLD signal changes, and TSPO PET imaging detect heightened dorsal‑horn activity and glial activation, providing objective evidence of central sensitization.
Pathophysiology of Pain (PDF) – Chronic pain starts with peripheral sensitization driven by inflammatory mediators and ion‑channel dysregulation, then spreads to spinal and supraspinal circuits via NMDA‑mediated wind‑up, glial cytokines, and loss of inhibitory control. Our patient‑friendly PDF explains these steps and how targeted physical‑therapy interventions can interrupt them.
Central Sensitization & Neuropathic Pain – Hyper‑responsive spinal neurons amplify normal inputs, often co‑existing with neuropathic pain from damaged nerves. NMDA receptors, P2X4 microglia, and BDNF sustain this state. Graded exposure, manual desensitization, and education restore normal modulation.
Neuropathic Pain – Originating from nerve damage, it presents as burning, electric‑shock, or tingling sensations with allodynia. PT reduces hypersensitivity through graded desensitization, functional movement retraining, and strengthening.
Neuropathic Chronic Pain – Persistent months‑to‑years after injury, it requires a multimodal approach: manual therapy for tissue mobility, graded activity for safe functional use, and neuro‑education to empower patients to modulate pain signals.
4. Evidence‑Based Physical‑Therapy Interventions
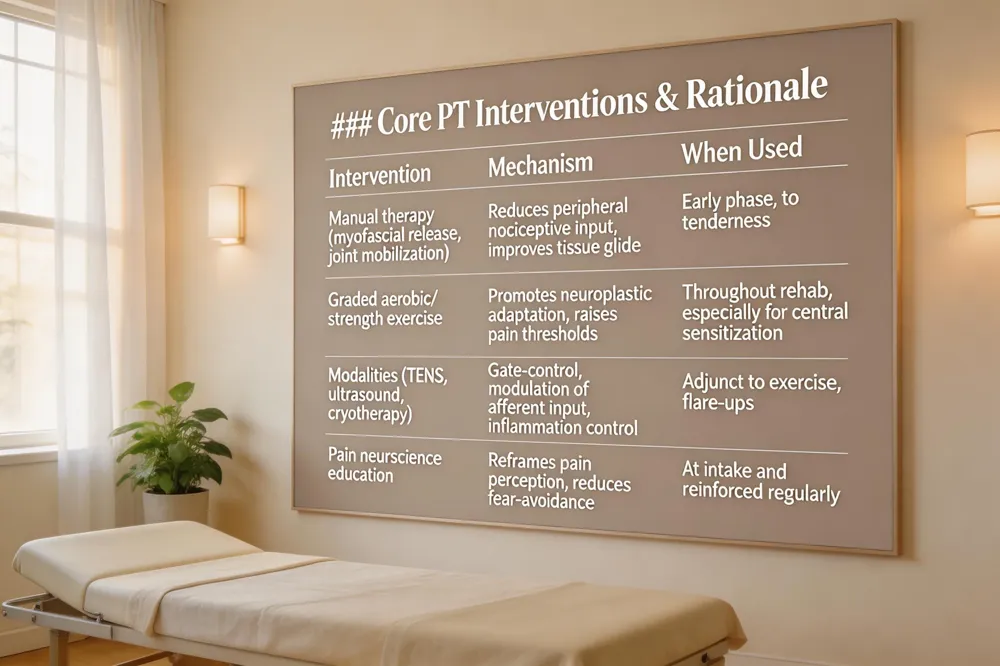 | ||
| Physical therapists begin by evaluating movement patterns, posture, and functional limits to identify pain generators. Hands‑on manual therapy—myofascial release, joint mobilizations, and dry needling—restores tissue glide, reduces nerve irritation, and lowers peripheral sensitization. |
{kind=link}
Therapeutic exercise follows a graded‑exposure model. Low‑impact aerobic activity and progressive strength training promote neuroplastic adaptation, increase pain thresholds, and normalize central nervous system excitability.
Adjunctive modalities such as TENS, therapeutic ultrasound, and cryotherapy temporarily modulate afferent input, interrupt nociceptive signaling, and improve local blood flow, supporting the desensitization process.
Patient education is integral. Pain neuroscience education explains how pain arises from sensitized nervous tissue rather than ongoing tissue damage, reducing fear‑avoidance behaviors and empowering self‑management.
What do physical therapists do for pain? They assess biomechanics, apply manual techniques, prescribe graded exercise, use modalities to modulate pain signals, and educate patients on body mechanics and coping strategies.
Pain management physiotherapy PPT outlines pain classifications, physiology, assessment tools, and evidence‑based interventions—including manual therapy, exercise, modalities, and education—to set functional goals and monitor outcomes.
Central sensitization treatment combines gentle mobilizations to cut peripheral input, aerobic/strength programs for neuroplastic change, neuro‑education, and cognitive‑behavioral strategies to restore balanced central processing.
Neuroinflammation and central sensitization in chronic pain are driven by activated spinal glia releasing cytokines that heighten neuronal excitability. Physical therapy counters this through graded movement, manual therapy, and education that reduce nociceptive drive, modulate glial activity, and enhance endogenous inhibitory pathways.
5. Specific Pain Conditions and Tailored PT Strategies
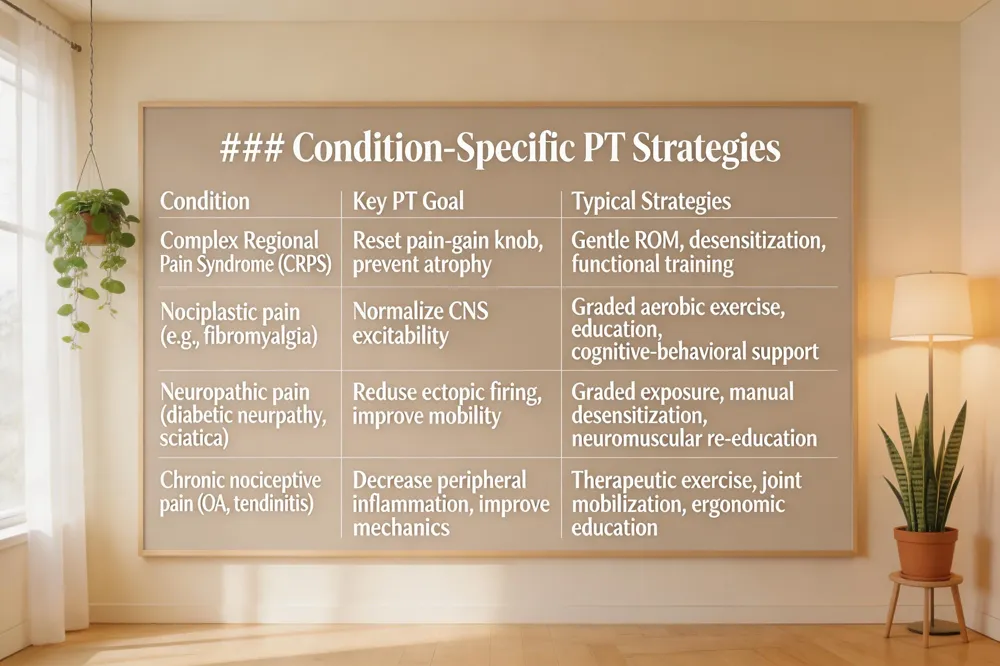 | ||
| Neuropathic conditions such as diabetic neuropathy, post‑herpetic neuralgia, and sciatica arise from lesions to the somatosensory system. Physical therapy (PT) addresses the maladaptive plasticity that drives ectopic firing and central sensitization by using graded exposure, manual desensitization, and neuromuscular re‑education to restore normal movement patterns and diminish pain‑amplifying signals. |
{kind=link}
Complex regional pain syndrome (CRPS) – CRPS is a chronic, often post‑traumatic disorder marked by burning pain, swelling, temperature and skin changes, and extreme touch sensitivity. Early PT intervention is essential. A therapist will employ gentle range‑of‑motion exercises, desensitization techniques, and functional training to prevent muscle atrophy, improve circulation, and gradually reset the nervous system’s pain‑gain knob.
Nociplastic pain – This type of pain stems from central sensitization rather than tissue damage. Patients experience widespread pain, fatigue, sleep disruption, and heightened sensory sensitivity. PT focuses on pain neuroscience education, graded aerobic and strengthening exercise, and cognitive‑behavioral strategies to retrain the brain’s interpretation of sensory input and strengthen descending inhibitory pathways.
Pathological pain examples – Include neuropathic disorders (e.g., diabetic neuropathy, trigeminal neuralgia), central‑sensitization syndromes such as fibromyalgia, cancer‑related pain, and CRPS. PT interventions target both peripheral drivers (manual therapy, scar mobilization) and central mechanisms (graded exposure, aerobic conditioning) to reduce hyper‑excitability.
Chronic nociceptive pain examples – Osteoarthritis, chronic low‑back pain, post‑traumatic arthritis, tendinitis, bursitis, and posture‑related neck/shoulder strain fall into this category. PT employs therapeutic exercise, joint mobilization, and ergonomic education to lower inflammatory mediators, improve joint mechanics, and prevent the transition to central sensitization.
Central sensitization syndrome vs. fibromyalgia – Central sensitization syndrome (CSS) describes the neurophysiologic state of heightened CNS responsiveness that can affect multiple organ systems. Fibromyalgia is a prototypical CSS condition, defined by widespread musculoskeletal pain plus fatigue, sleep problems, and “fibro‑fog.” While CSS is a broader concept encompassing conditions such as irritable bowel syndrome and chronic fatigue syndrome, fibromyalgia has specific diagnostic criteria and is identified after other causes are excluded. PT programs for CSS and fibromyalgia share core components: education, graded movement, and psychosocial support, aiming to normalize pain processing and improve functional outcomes.
6. Frequently Asked Questions – Quick Answers for Patients
 | |
| Most common reasons for physical therapy – Patients seek PT for musculoskeletal injuries, joint pain, post‑surgical rehabilitation, chronic back or neck pain, arthritis, sports‑related strains, and balance or fall‑prevention programs. Neurological conditions (stroke, peripheral neuropathy), pelvic‑floor dysfunction, TMD, and chronic health issues such as COPD or fibromyalgia also drive referrals. |
{kind=link}
Pain‑management physical therapy near me – Our La Crosse clinic offers personalized care that blends manual therapy, therapeutic exercise, and evidence‑based modalities (ultrasound, electrical stimulation, cryotherapy). Each plan targets the source of discomfort, restores mobility, and supports long‑term wellness.
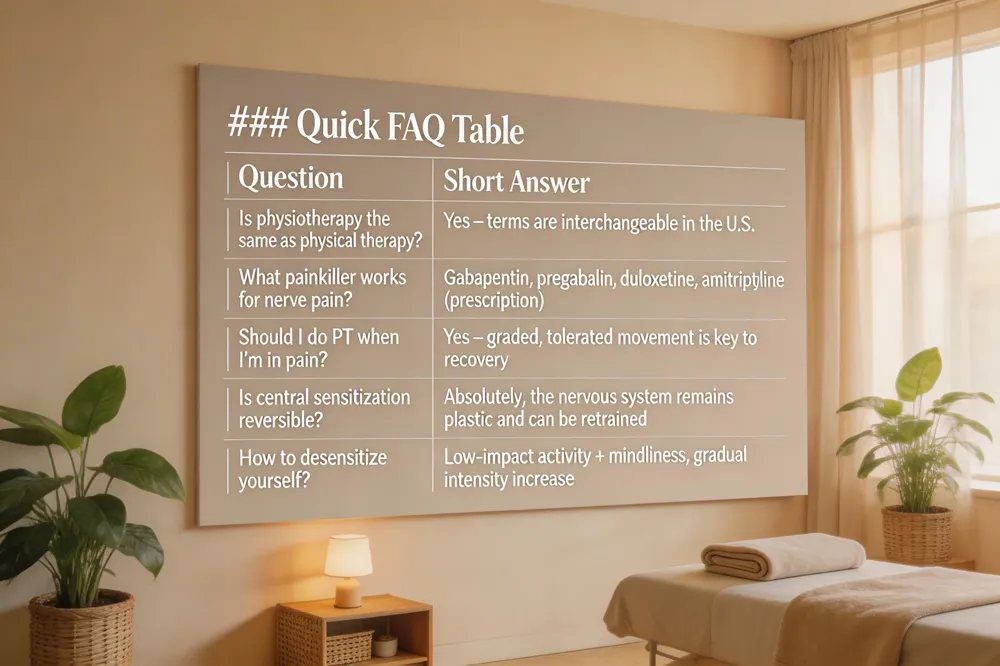
Is physiotherapy the same as physical therapy? – In the United States the terms are interchangeable. Both refer to licensed professionals who assess, diagnose, and treat movement‑related problems using manual techniques, exercise, and education.
What is a good painkiller for nerve pain? – OTC NSAIDs may help mild cases, but prescription agents such as gabapentin, pregabalin, duloxetine, or amitriptyline are more effective for neuropathic pain. Topical lidocaine or capsaicin can also provide localized relief.
Should you do physical therapy when in pain? – Yes. PT is a drug‑free, evidence‑based way to reduce pain, improve function, and prevent chronic sensitization through graded, tolerated movement.
How long does pain last after an injury? – Mild strains resolve in 48–72 hours; moderate sprains last 1–2 weeks; severe injuries can persist for weeks or months without proper treatment.
Is central sensitization reversible? – Absolutely. The nervous system remains plastic. Targeted graded exposure, gentle movement, pain‑reprocessing therapy, and education can normalize hyper‑excitable pathways.
How to desensitize yourself to pain? – Begin with low‑impact activities (walking, swimming, gentle stretching) combined with deep breathing or mindfulness. Gradually increase intensity while pacing to avoid flare‑ups, allowing the nervous system to reset its alarm response.
7. Practical Tips for Managing Pain at Home
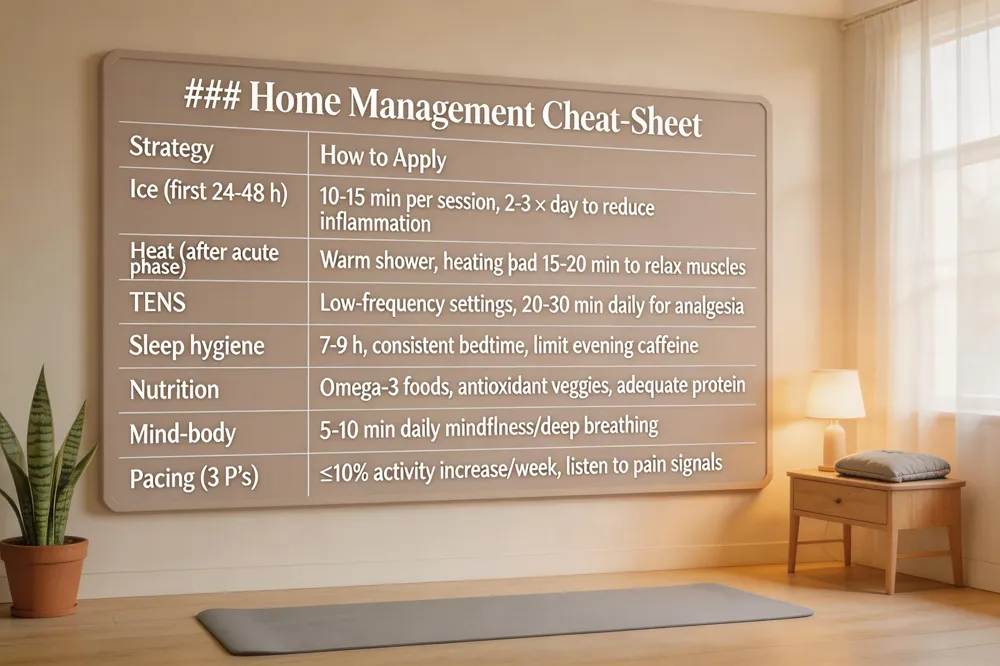 | |
| Self‑care strategies – Simple modalities such as heat, ice, and a low‑intensity TENS unit can dampen nociceptive input without masking the nervous system’s need to reset. Apply ice for the first 24‑48 hours after a flare to reduce inflammation, then switch to gentle heat or a warm shower to improve blood flow and relax muscle tension. A TENS device delivers mild electrical pulses that activate large‑diameter fibers, closing the "gate" to pain signals and promoting endorphin release. |
{kind=link}
Sleep hygiene and nutrition – Adequate restorative sleep stabilizes descending inhibitory pathways, while a balanced diet rich in omega‑3 fatty acids, antioxidant vegetables, and adequate protein supports neurotransmitter synthesis and reduces neuroinflammation. Aim for 7‑9 hours of sleep, keep a consistent bedtime, and limit caffeine late in the day.
Mind‑body practices – Mindfulness, deep‑breathing, and guided imagery lower stress hormones that amplify central sensitization. Even a few minutes of focused breathing before activity can reset the brain‑spinal cord circuitry and improve pain thresholds.
Gradual activity pacing – The 3 P’s of pain management—Pacing, Patience, Persistence—guide safe progression. Begin with low‑impact movements (e.g., walking, gentle stretching) and increase duration by no more than 10 % each week. Consistency builds confidence while protecting the nervous system from overload.
Key quick answers
- Central sensitization natural treatment: Gentle graded activity, mindfulness, good sleep, and nutrition retrain the nervous system.
- 3 P’s of pain: Pacing, Patience, Persistence.
- 4 P’s of chronic pain: Pain, Purpose, Pacing, Positivity.
- 5 A’s of chronic pain: Analgesia, Activities of daily living, Adverse effects, Affect, Aberrant drug‑related behaviors.
- 5 mechanisms of pain: Central sensitization, peripheral neuropathic pain, nociceptive pain, sympathetically maintained pain, cognitive‑affective pain.
- Central sensitization medication: Duloxetine, low‑dose tricyclics, gabapentin, pregabalin.
- Physiotherapy pain‑relief machine: TENS, therapeutic ultrasound, EMS – all used to modulate pain signals and promote healing.
8. Take the Next Step – Personalized Care at O’Brien Physical Therapy
 | |
| O’Brien Physical Therapy in La Crosse, Wisconsin, offers a community‑focused, evidence‑based approach to chronic pain. Our clinic combines state‑of‑the‑art manual therapy, therapeutic exercise, and modalities such as ultrasound, electrical stimulation, and cryotherapy to reduce neural sensitization and restore function. |
{kind=link}
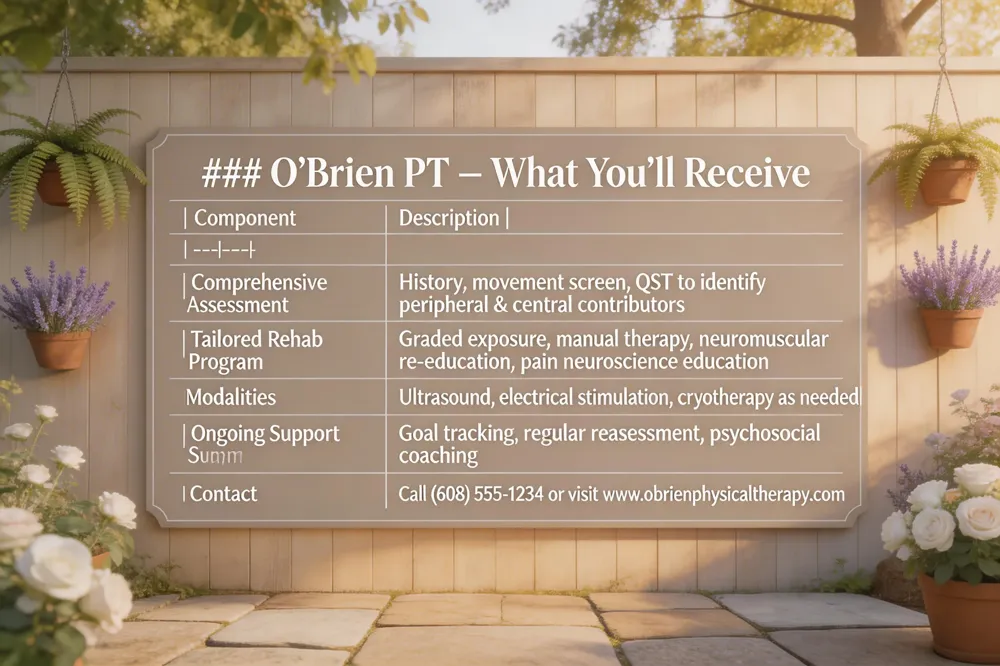
Comprehensive Assessment – Every new patient undergoes a detailed history, movement screen, and quantitative sensory testing to identify peripheral sensitization and central sensitization, fear‑avoidance behaviors, and functional deficits. We use this data to pinpoint the exact contributors to pain and to set realistic, patient‑driven goals.
Tailored Rehabilitation Programs – Based on the assessment, we design individualized plans that may include graded exposure, neuromuscular re‑education, myofascial release, and pain neuroscience education. The goal is to normalize nociceptive input, promote adaptive neuroplasticity, and empower patients to move confidently.
Contact Information – Call (608) 555‑1234 or visit www.obrienphysicaltherapy.com to schedule your initial evaluation. Our friendly staff will help you start a personalized pathway toward lasting pain relief and optimal wellness.
Answer to “Pain management physical therapy near me” – Our La Crosse clinic provides personalized pain‑management physical therapy that combines manual therapy, therapeutic exercise, and evidence‑based modalities such as ultrasound, electrical stimulation, and cryotherapy to reduce pain and restore function. We assess each patient individually and design a customized treatment plan that targets the source of discomfort, improves mobility, and supports long‑term wellness.
Conclusion: Rewiring the Nervous System for a Pain‑Free Life
Neural sensitization—whether peripheral or central—is not a permanent verdict. The nervous system retains remarkable plasticity, and research shows that the heightened excitability underlying chronic pain can be "de‑sensitized" through systematic, evidence‑based interventions. Physical therapy in La Crosse provides precisely those tools: graded exposure to movement, manual techniques that restore normal proprioceptive input, therapeutic exercise that activates descending inhibitory pathways, and pain‑neuroscience education that reshapes threat perceptions. Each session is individualized, beginning with an assessment of sensitization signs (e.g., allodynia, lowered pressure‑pain thresholds) and progressing at a pace that respects the patient’s comfort while gently expanding the pain‑free movement envelope. By combining gentle loading, neuromodulatory modalities such as TENS, and mindfulness‑based strategies, we help the dorsal‑horn and brain circuits re‑establish balanced signaling, ultimately reducing hyper‑excitability and the fear‑avoidance cycle. If you live in the La Crosse community and are experiencing lingering pain after an injury has healed, consider scheduling a comprehensive evaluation with our clinic. Together we can design a personalized rehabilitation plan that targets the root mechanisms of sensitization, empowers you to reclaim function, and moves you closer to a truly pain‑free life.